How Digital HEDIS® is Powering the Shift to Value Based Care
By Karen Manning, MBA, BSN, RN, Director, Business Solutions
In our earlier blogs, we explored why manual chart abstraction is giving way to digital HEDIS and how CMS rules are creating the data conditions for that shift. Those regulatory and technical changes matter, but they are not the end goal. The real driver is the steady move toward value-based care.
As value-based models expand, plans and providers are being asked not only to improve quality but to prove it. That means measurement must evolve. It must be faster, more accurate, more collaborative, and embedded inside care delivery rather than layered on after the fact. That is where digital HEDIS fits.
The rise of value-based care
CMS frames value-based care around quality, provider performance, and patient experience. The Affordable Care Act accelerated adoption of alternative payment models and private payers followed suit. Patients and employers pressed for transparency and better experience. Over time, fee-for-service incentives misaligned with clinical and financial goals, and the industry began rewarding outcomes and coordination.
Today, several payment approaches are in wide use:
- Pay for performance: A portion of payment is tied to meeting agreed quality and efficiency targets.
- Shared savings: Providers share savings when they meet cost and quality benchmarks.
- Bundled payments: One payment covers a defined episode of care, encouraging coordination across settings.
- Full or partial capitation: Fixed per-member, per-month payment that rewards proactive, efficient care within a budget.
Every model relies on timely, accurate data. Without it, teams cannot track performance reliably, share risk confidently, or target interventions at the right time.
| Model | What it incentivizes |
|---|---|
| Pay for performance | Meeting defined quality metrics |
| Shared savings | Delivering care below target cost while maintaining quality |
| Bundled payments | Coordinating a full episode of care |
| Full or partial capitation | Efficient, proactive care per member per month |
Why data sharing is the foundation
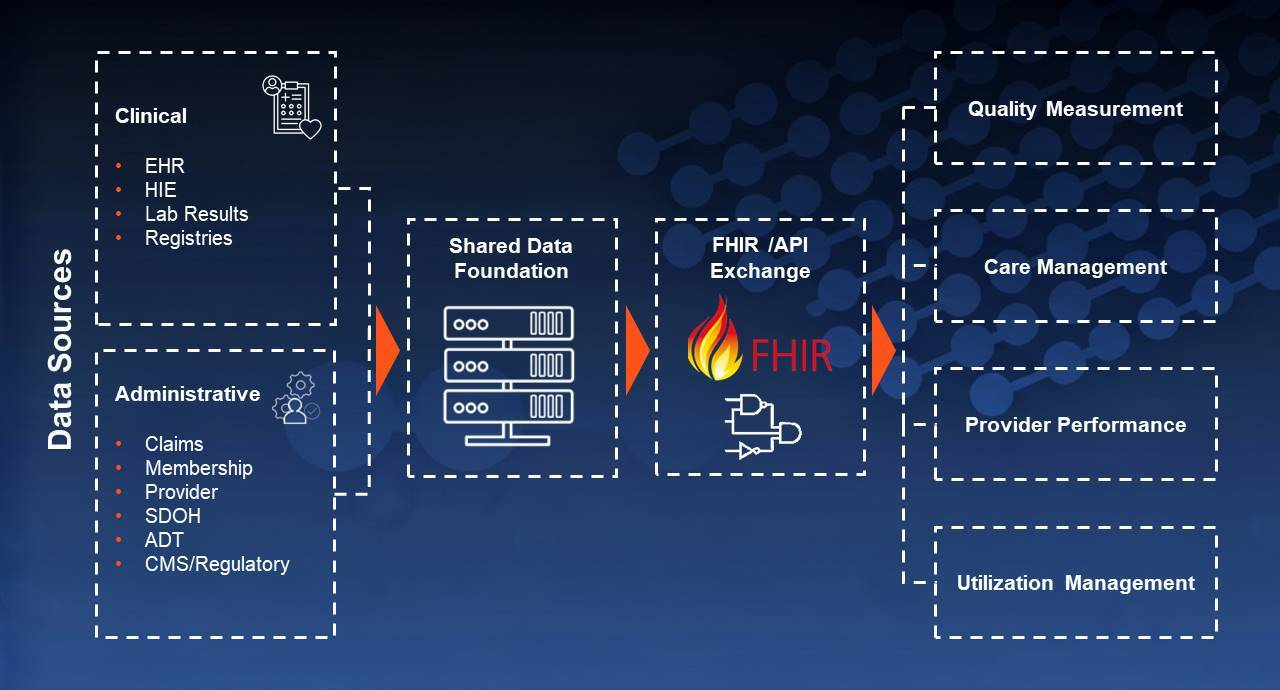
Value-based care depends on a shared and current view of performance across payers and providers. Practically, that requires more than general “infrastructure.” It requires a working fabric that can:
- Build a governed, longitudinal member record that unifies clinical, claims, and encounter data.
- Represent measures and clinical artifacts in standardized, computable formats.
- Exchange data in both directions using FHIR-based APIs so updates are timely and reusable.
- Enforce role-based access, consent, audit trails, and provenance to maintain trust and compliance.
- Return feedback to providers in a form they can use during the encounter, not weeks later.
With those pieces in place, both sides can see the same measure status, coordinate outreach while it still matters, close gaps earlier, and align incentives without abrasion caused by stale or incomplete data.
The traditional HEDIS process has been retrospective and claims heavy. A preventive test completed today might not change the reported rate for one or two months. That lag erodes trust and delays action. A modern, shared data foundation narrows that gap, supports bidirectional communication, and makes improvement work part of daily practice.

How digital HEDIS supports value-based care
NCQA is steering the industry toward fully digital measurement. By Measurement Year 2029, all HEDIS measures are expected to be captured digitally for reporting in 2030. In that world, the process changes from seasonal abstraction to continuous measurement supported by computable data.
Digital HEDIS strengthens value-based care in three practical ways:
- Timeliness: Data flows enable more current measure status and faster outreach.
- Consistency: Standardized specifications reduce ambiguity and support fair comparisons.
- Collaboration: Bidirectional exchange lets providers see feedback where they work, which promotes shared problem-solving rather than end-of-year disputes.
Digital HEDIS does not succeed in a silo. Quality teams, utilization management, care management, provider relations, and IT need to align on common definitions, shared workflows, and clear governance, so data moves with the work, and everyone trusts the results.
Operational realities leaders should plan for
Moving from manual to digital measurement is less about a single technology decision and more about operating discipline. Leaders who make durable progress tend to:
- Map how clinical data enters and moves across the plan, from ingestion to normalization to use in quality, utilization, and care management.
- Decide on canonical definitions for member identity, attribution, and event timing so measures compute the same way across teams.
- Plan for change management with providers and internal staff. Timely feedback is only helpful if it is visible and usable in existing workflows.
- Govern the data explicitly, including consent, provenance, access controls, and audit trails, so reuse is safe and trusted.
- Sequence the work so CMS interoperability tasks and digital HEDIS enable one another rather than compete for resources.
What quality leaders should focus on now
Across this series, we have looked at HEDIS transformation from several angles:
- Blog 1 examined the limits of manual abstraction and why NCQA’s digital mandate is reshaping how quality is measured.
- Blog 2 showed how CMS interoperability and prior authorization rules are building the infrastructure for near real-time, digital measurement.
- This blog connects those changes to strategy by linking digital HEDIS to the demands of value-based care.
Taken together, these shifts point to a clear conclusion. Success in digital HEDIS and value-based care requires modern data foundations, continuous flow of clinical data, seamless exchange with providers, and operational alignment across quality, clinical, and IT teams, supported by strong governance.
Quick readiness check
Use these questions to assess your digital quality roadmap:
How Abacus helps
At Abacus, we help health plans create a foundation of usable, governed data. Our platform ingests clinical data at scale, normalizes and converts it to FHIR, and supports bidirectional exchange so you can operationalize digital quality measures for HEDIS and across CMS quality programs. The same data foundation supports utilization management, care management, and provider feedback so improvement work is continuous and shared.
Next step
If you are still addressing some of the readiness items or you are not sure where to start, you are not alone. Whether you are refining existing systems or building new ones, we can help you move forward with confidence.